Both contain psilocybin. Both can catalyse profound inner experiences. But in the Netherlands, one is legally available, professionally cultivated, and used in guided retreats, private sessions and in informal settings — while the other is not. Understanding why matters for anyone curious about what these substances actually are and what the research says about their potential.
By Naomi Stubbé and Francisca Niklitschek
A Fungus With Two Forms
If you have heard of psilocybin — the compound at the centre of a significant and growing body of clinical research into depression, anxiety, and psychological change — you may have encountered it in one of two forms: magic mushrooms or magic truffles. The names suggest two different things. In biological terms, they are two different expressions of the same organism. In pharmacological terms, they contain the same active molecule. In legal terms, at least in the Netherlands, only one of them is permitted.
The magic truffle — or sclerotium, to use its correct biological term — is not a different substance from the magic mushroom. It is a different growth stage of the same fungal organism: one that develops underground rather than above it, and that has, through a combination of botanical classification and Dutch regulatory specificity, retained a legal status that the above-ground mushroom lost in 2008. Sclerotia are underground masses of fungal filaments that store nutrients and help the fungus survive during drought or cold — and in the Netherlands, they are cultivated and openly sold precisely because they fall outside the legislation that banned mushrooms. For anyone curious about psilocybin, whether from a scientific perspective or a more personal one, understanding this distinction is a useful starting point (Stubbé, 2025).
This article explores what these two forms of psilocybin fungi actually are, how they compare in terms of chemistry, potency, and effect, how the Netherlands became a place where they are openly and legally available, and what the growing body of clinical research on psilocybin suggests about why any of this matters.
What Is the Difference? Botany Before Pharmacology
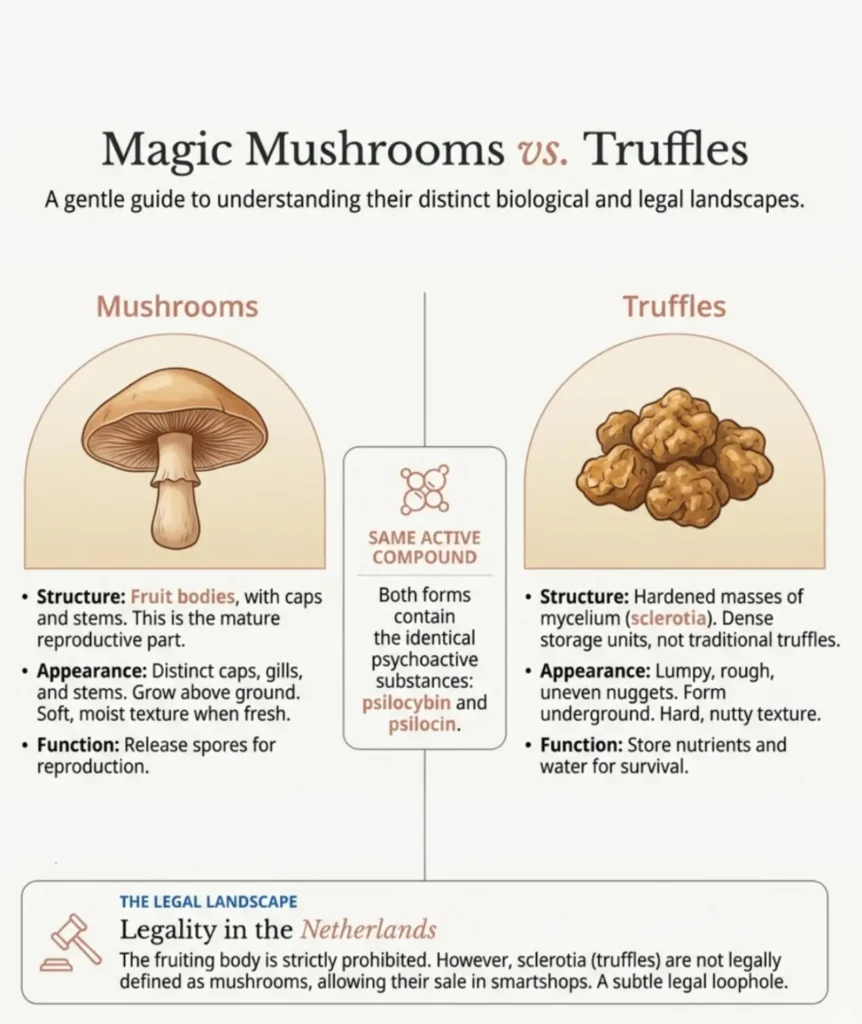
A magic mushroom is the fruiting body of a Psilocybe fungus — the visible, above-ground structure that the organism produces to spread spores. Several hundred species fall into this category worldwide. Well-known examples include Psilocybe cubensis (the Mexican mushroom), Psilocybe semilanceata (the liberty cap, native to European grasslands), and Psilocybe azurescens, found along the Pacific Northwest coast of North America (Stamets, 1996).
A magic truffle, by contrast, is a sclerotium — a hardened, dense mass of mycelium that forms underground. Sclerotia are not the reproductive structure of the fungus; they are its survival mechanism. When environmental conditions become hostile — drought, cold, nutrient depletion — certain Psilocybe species consolidate their mycelial energy reserves into these compact subterranean bodies. Only a handful of species reliably produce sclerotia, among them Psilocybe tampanensis (the original ‘Philosopher’s Stone’), Psilocybe mexicana, Psilocybe atlantis, and a cultivated variety known as Psilocybe hollandia, developed specifically for the Dutch market (Doubleblind, 2022; Wikipedia: Sclerotium).
The confusion between the two forms is understandable. In everyday language, both are commonly called ‘magic mushrooms.’ In biological terms, they are two different growth stages of the same organism — one produced above ground, one below. The critical point, pharmacologically speaking, is that both contain the same active compounds.
The Active Compound: Psilocybin and Its Mechanism
Whether it comes from a dried mushroom cap or a fresh truffle, the psychoactive molecule in both is psilocybin — a naturally occurring tryptamine alkaloid first isolated and identified by the Swiss chemist Albert Hofmann in 1958, working on samples of Psilocybe mexicana sent from Mexico by mycologist Roger Heim (Hofmann et al., 1958).
After ingestion, psilocybin is rapidly converted by the body into psilocin, the compound that actually crosses the blood-brain barrier and produces psychedelic effects. Psilocin is a close structural analogue of serotonin, and it binds with particular affinity to the 5-HT2A serotonin receptor — the same receptor that distinguishes all the classical psychedelics from other psychoactive substances (Passie et al., 2002; Nichols, 2004).
The consequence of this receptor binding is a cascade of changes across the brain’s large-scale networks. Most significantly, psilocybin disrupts activity in what neuroscientists call the Default Mode Network (DMN) — a cluster of interconnected brain regions associated with self-referential thought, rumination, memory retrieval, and the maintenance of the ordinary sense of self. Under normal conditions, the DMN is one of the most active and metabolically expensive systems in the brain. Under psilocybin, its connectivity decreases markedly, while connections between otherwise segregated brain networks increase. The result is a temporary state of heightened neural integration — what some researchers have described as increased ‘brain entropy’ — associated with the dissolution of habitual thought patterns and the emergence of novel perceptual and cognitive states (Carhart-Harris et al., 2012; 2017).
Research by Robin Carhart-Harris and colleagues at Imperial College London, as well as at Johns Hopkins University under Roland Griffiths, has consistently linked this DMN disruption not only to the immediate phenomenology of the psychedelic experience, but to lasting changes in brain connectivity and psychological flexibility that can persist for weeks after a single session (Carhart-Harris et al., 2018; Smigielski et al., 2019). A 2022 analysis by Daws and colleagues found that psilocybin therapy reduced depressive symptoms for up to six weeks after treatment, with effects linked to increased integration between brain networks.
Comparing Potency: The Role of Moisture
Both forms contain psilocybin as their primary active compound. When ingested, the body converts it to psilocin, which crosses the blood-brain barrier and produces psychedelic effects. The mechanism is identical regardless of whether the psilocybin comes from a dried mushroom or a fresh truffle.
The practical difference in dose comes almost entirely from moisture. Dried mushrooms typically retain only 5–10% of their original weight as water — meaning that psilocybin is relatively concentrated per gram. Fresh truffles, by contrast, contain roughly 70% water. As a general guide, 1 gram of dried mushroom corresponds approximately to 10 grams of fresh truffle. This simple ratio accounts for most of the perceived difference in potency: you need considerably more truffle by weight to reach a comparable effect, not because the compound is weaker, but because there is far more water in the product.
Commercially cultivated truffles in the Netherlands also offer something that home-grown or wild mushrooms often do not: relative consistency. Because they are produced under controlled conditions in professional facilities, batch-to-batch variation is lower than with dried mushrooms, where potency can swing considerably depending on growing conditions, drying methods, and whether one is consuming caps (typically higher concentration) or stems (lower). For those approaching psilocybin with care and intention — particularly in a guided context — this predictability is a meaningful practical advantage.
The Dutch Legal Framework: Why Truffles Are Legally Available
The Netherlands has maintained one of Europe’s most pragmatic drug policy frameworks for several decades — an approach grounded in harm reduction rather than prohibition. This philosophy, holds that regulation and public health information are more effective tools than criminalisation for managing the risks associated with psychoactive substances. It is the same framework that produced the cannabis coffee shop system, and it has historically been accompanied by some of the lowest drug-related harm statistics in Europe (Wikipedia: Drug Policy of the Netherlands).
Within this framework, psilocybin-containing mushrooms were openly and legally sold in Dutch smartshops — the retail outlets specialising in legal psychoactive herbs, supplements, and related products — through the 1990s and into the 2000s. Health authority assessments during this period found no significant public health risk from their regulated sale. In 2008, however, the Dutch government moved to ban psychoactive mushrooms, adding over a hundred Psilocybe species to List II of the Opium Act.
Crucially, the legislation was specifically directed at mushrooms — the above-ground fruiting bodies. Sclerotia were not mentioned. Since sclerotia are recognised in botanical and mycological science as a structurally distinct growth form from the mushroom fruiting body, they remained outside the legislation.
The result is that psilocybin truffles are today fully legal in the Netherlands — available for purchase in regulated smartshops, produced by commercial farms operating openly and transparently, and used in professional guided retreat settings. For those approaching psilocybin with genuine curiosity and care, this legal clarity matters. It means that access is not dependent on grey markets, unverified sources, or legal ambiguity. The supply chain is visible, the products are professionally produced, and the context — when chosen carefully — can be one of proper preparation and support.
Psilocybin in Clinical Research: The Evidence Base
It is worth noting that the clinical research which has generated global interest in psilocybin over the past two decades has, for the most part, used either synthetic psilocybin or mushroom-derived psilocybin rather than truffle preparations. This matters for interpretation: the research results are not about truffles specifically, but about psilocybin.
The evidence is substantial and growing. A 2016 study by Carhart-Harris and colleagues at Imperial College London found that two high doses of psilocybin, combined with psychological support, produced rapid and significant reductions in depressive symptoms in patients with treatment-resistant depression — with effects persisting at six-month follow-up (Carhart-Harris et al., 2016; 2018). A 2020 randomized controlled trial published in JAMA Psychiatry by Davis and colleagues at Johns Hopkins reported that two psilocybin sessions produced large, rapid, and durable decreases in depression and anxiety scores. A 2021 randomized trial by Carhart-Harris and colleagues comparing psilocybin to the SSRI escitalopram found comparable antidepressant effects, with psilocybin additionally associated with improvements in emotional processing and well-being (Carhart-Harris et al., 2021).
Research published in the Journal of Psychopharmacology has reported that psilocybin produces lasting changes in psychological well-being, including increases in measures of openness, connectedness, and life meaning — effects that participants often describe as among the most personally significant experiences of their lives (Griffiths et al., 2008; 2016). A notable study by Hasler and colleagues documented lasting metabolic changes in brain regions associated with emotional processing following a single psilocybin dose (Hasler et al., 2004).
The neuroplasticity effects of psilocybin — its ability to promote synaptic growth and the formation of new neural connections — are increasingly understood as a central mechanism of its therapeutic potential. Research at Yale and other institutions has shown that psilocybin promotes structural neuroplasticity in the prefrontal cortex, a region implicated in emotional regulation and cognitive flexibility (Ly et al., 2018). This neuroplastic window, which opens acutely during the experience and may persist for days to weeks afterward, is thought to underlie psilocybin’s capacity to facilitate psychological change that outlasts the session itself.
Conclusion
Magic truffles and magic mushrooms are, at the molecular level, the same thing: two biological forms of certain Psilocybe species, both containing psilocybin, both producing psilocin in the body, both engaging the same serotonergic mechanisms in the brain. The differences between them are structural (above-ground fruiting body versus below-ground sclerotium), pharmacokinetic (slightly different onset profiles and dose equivalents), and — crucially in the Dutch context — legal.
The growing body of research on psilocybin suggests that the molecule, delivered in an appropriate context with adequate preparation and integration, has genuine and lasting effects on how the brain processes emotion, self-concept, and behavioural patterns.
The fact that this experience is accessible legally in the Netherlands, through truffles rather than mushrooms, is partly historical accident and partly the consequence of a country that has, over several decades, chosen to regulate rather than prohibit. That choice created the conditions for a legitimate industry, and for a generation of practitioners who have developed real expertise in supporting people through experiences that the clinical literature increasingly describes as genuinely significant — not only for mental health, but for how people relate to their own inner lives.
Disclaimer
This article is intended for informational and educational purposes only. It does not constitute medical or psychological advice. If you are experiencing mental health difficulties or considering any therapeutic intervention, please consult a qualified healthcare professional.
References
- Pellegrini, M., Rotolo, M.C., Marchei, E., Pacifici, R., Saggio, F., & Pichini, S. (2013). Magic truffles or Philosopher’s stones: a legal way to sell psilocybin? Drug Testing and Analysis, 5(3), 182–185. https://doi.org/10.1002/dta.1400
- Passie, T., Seifert, J., Schneider, U., & Emrich, H.M. (2002). The pharmacology of psilocybin. Addiction Biology, 7(4), 357–364. https://pubmed.ncbi.nlm.nih.gov/14578010/
- Hofmann, A., Heim, R., Brack, A., & Kobel, H. (1958). Psilocybin, a psychotropic substance from the Mexican mushroom Psilocybe mexicana Heim. Experientia, 14(3), 107–109.
- Carhart-Harris, R.L., et al. (2012). Neural correlates of the psychedelic state as determined by fMRI studies with psilocybin. Proceedings of the National Academy of Sciences, 109(6), 2138–2143. https://www.pnas.org/doi/10.1073/pnas.1119598109
- Carhart-Harris, R.L., et al. (2017). Psilocybin for treatment-resistant depression: fMRI-measured brain mechanisms. Scientific Reports, 7, 13187. https://doi.org/10.1038/s41598-017-13282-7
- Carhart-Harris, R.L., et al. (2021). Trial of psilocybin versus escitalopram for depression. New England Journal of Medicine, 384, 1402–1411. https://doi.org/10.1056/NEJMoa2032994
- Smigielski, L., Scheidegger, M., Kometer, M., & Vollenweider, F.X. (2019). Psilocybin-assisted mindfulness training modulates self-consciousness and brain default mode network connectivity with lasting effects. NeuroImage, 196, 207–215. https://doi.org/10.1016/j.neuroimage.2019.04.009
- Griffiths, R.R., et al. (2008). Mystical-type experiences occasioned by psilocybin mediate the attribution of personal meaning and spiritual significance 14 months later. Journal of Psychopharmacology, 22(6), 621–632. https://doi.org/10.1177/0269881108094300
- Griffiths, R.R., et al. (2016). Psilocybin produces substantial and sustained decreases in depression and anxiety in patients with life-threatening cancer. Journal of Psychopharmacology, 30(12), 1181–1197. https://doi.org/10.1177/0269881116675513
- Davis, A.K., et al. (2021). Effects of psilocybin-assisted therapy on major depressive disorder. JAMA Psychiatry, 78(5), 481–489. https://doi.org/10.1001/jamapsychiatry.2020.3285
- Ly, C., et al. (2018). Psychedelics promote structural and functional neural plasticity. Cell Reports, 23(11), 3170–3182. https://doi.org/10.1016/j.celrep.2018.05.022
- Stamets, P. (1996). Psilocybin Mushrooms of the World: An Identification Guide. Ten Speed Press.
- Wikipedia: Drug Policy of the Netherlands. https://en.wikipedia.org/wiki/Drug_policy_of_the_Netherlands
- Wikipedia: Sclerotium. https://en.wikipedia.org/wiki/Sclerotium
- Daws, R.E., et al. (2022). Increased global integration in the brain after psilocybin therapy for depression. Nature Medicine, 28, 844–851. https://doi.org/10.1038/s41591-022-01744-z
- 16. Stubbé, Naomi. (2025). The Potential of Psychedelics [Het potentieel van psychedelica]. (Original Dutch publication; relevant sections on inner healing intelligence, guide competencies, and the role of trust in psychedelic sessions.)


